Temozolomide (Temodar) for Brain Metastases
http://cancergrace.org/cancer-tr ... dar-for-brain-mets/
Historically, chemotherapy has had a relatively minor role in the management of brain metastases. Although there is a rather low response rate in the brain from some standard lung cancer chemo regimens, we generally conclude that most of our chemo canвҖҷt be too effective in the brain because of the blood-brain barrier (BBB) that is relatively impermeable to the majority of our commonly used chemo agents (there is some debate about whether the metastases disrupt that barrier and can allow other chemo agents to get into the brain, but thatвҖҷs still a murky issue). However, some of the drugs that are routinely used to treat primary brain tumors (cancers that start in the brain tissue) can get through the BBB and reach significant concentrations that can effectively fight cancer. One of the agents that has been shown to be valuable in treating primary brain tumors is temozolomide, or Temodar, an oral chemotherapy drug that is given with radiation to the brain and also on its own off of radiation. Because itвҖҷs been shown to improve survival for patients with tumors that start in the brain, and is also helpful for patients with metastatic melanomas, itвҖҷs also been an agent that has been the focus of research questioning whether it can improve results when added to radiation, or potentially on its own, in patients with brain metastases from solid tumors like lung cancer.
While there havenвҖҷt been enough studies of temodar in the treatment of brain metastases to establish a role for it in this setting, the limited studies that have been done have looked encouraging. On its own, if given without whole brain radiation therapy (WBRT), the studies that have been done (abstracts here and here and here, for example) have included a few dozen patients, most or all on these studies having previously received WBRT, and have shown partial response rates (brain metastasis shrinkage) in the single digits, no complete responses, but sometimes with up to about half the patients with stable disease in the brain for several months (although itвҖҷs hard to know what to expect in terms of progression in the brain after WBRT). Importantly, itвҖҷs reaching for a pretty high bar to be looking for responses of heavily treated patients who have undergone WBRT for brain metastases and are now progressing. The main side effects of temodar were decreased blood counts, some liver test abnormalities, and sometimes nausea and fatigue.
Temodar has also been studied in combination with WBRT. In a study from Spain, Verger and colleagues (abstract here) randomized 85 patients with brain metastases (51% from lung cancer, by far the leading subgroup) to receive WBRT with or without temodar (75 mg/m2/day) during RT and then 200 mg/m2 on days 1-5 every 28 days for a couple of additional months. While the response rate was not significantly improved with temodar, at 90 days there was a better progression-free survival in the recipients of temodar + WBRT (72% vs. 54%), and a decreased risk of dying from brain metastases (69% vs. 41%). Another trial from Greece, by Antonadou and colleagues (abstract here), randomized 52 patients with brain mets (21 with lung cancer) to receive WBRT with or without concurrent temodar, followed by up to 6 cycles of temodar alone (for the first 5 days of each 28 day cycle). This smaller study showed a very high response rate of 96% in the patients who received the combination of temodar and WBRT, compared with 67% for WBRT alone (highly statistically significant), and also greater neurologic symptom improvement with the combination approach.
There are a range of studies being conducted now that are looking at temodar with radiation (list here), sometimes combined with or compared with other agents, especially EGFR inhibitors, since these have also been associated with responses of brain metastases (the subject of a future post). For now, the relatively small studies that have been done havenвҖҷt shown it to be a home run, but it looks like this is an agent on a rather short list of drugs that can have an impact on brain metastases, in combination with or following local approaches such as WBRT. Whether temodar can decrease risk of progression in the brain for patients who undergo stereotactic radiosurgery alone, or whether it is more effective when combined with other agents like tarceva, as is being studied, is still unknown right now.
|




 еҰҲеҰҲиӮәи…ә9е№ҙпјҢзҺ°еңЁиҝ·иҢ«иҜ·еӨ§зҘһи·ҜиҝҮз»ҷ
з—…жғ…еӨ§дҪ“д»Ӣз»ҚпјҢжӮЈиҖ…еҘізҺ°69е‘ЁеІҒпјҢжңүеҗёзғҹеҸІ50е№ҙпјҢ2003е№ҙж„ҹеҶ’жҶӢж°”пјҢCTжҳҫзӨәиӮәйғЁжңүзүҮзӮҺз—ҮпјҢ
еҰҲеҰҲиӮәи…ә9е№ҙпјҢзҺ°еңЁиҝ·иҢ«иҜ·еӨ§зҘһи·ҜиҝҮз»ҷ
з—…жғ…еӨ§дҪ“д»Ӣз»ҚпјҢжӮЈиҖ…еҘізҺ°69е‘ЁеІҒпјҢжңүеҗёзғҹеҸІ50е№ҙпјҢ2003е№ҙж„ҹеҶ’жҶӢж°”пјҢCTжҳҫзӨәиӮәйғЁжңүзүҮзӮҺз—ҮпјҢ
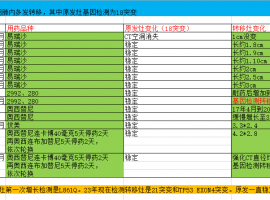
 L861QеӨҡеҸ‘и„‘иҪ¬е’Ңи„‘иҶңиҪ¬дҪҝз”ЁдҪҗеҲ©жӣҝе°ј
жӮЈиҖ…жҳҜжҲ‘еҰҲеҰҲпјҢд»Ҡе№ҙ71еІҒпјҢжІ»з–—з»ҸиҝҮеҰӮдёӢпјҡ
2023-6-7 зЎ®иҜҠеҸіиӮәдёҠеҸ¶иӮәи…әзҷҢдјҙеӨҡеҸ‘ж·Ӣе·ҙз»“гҖҒ
L861QеӨҡеҸ‘и„‘иҪ¬е’Ңи„‘иҶңиҪ¬дҪҝз”ЁдҪҗеҲ©жӣҝе°ј
жӮЈиҖ…жҳҜжҲ‘еҰҲеҰҲпјҢд»Ҡе№ҙ71еІҒпјҢжІ»з–—з»ҸиҝҮеҰӮдёӢпјҡ
2023-6-7 зЎ®иҜҠеҸіиӮәдёҠеҸ¶иӮәи…әзҷҢдјҙеӨҡеҸ‘ж·Ӣе·ҙз»“гҖҒ
 иғ¶иҙЁзҳӨж–°и‘Ҝ
ONC201жҳҜеӨҡе·ҙиғәD2/3еҸ—дҪ“пјҲDRD2/3пјүзҡ„йҖүжӢ©жҖ§жӢ®жҠ—еүӮпјҢиғҪеӨҹжңүж•Ҳең°йҖҸиҝҮиЎҖи„‘еұҸйҡңпјҢеҸӘж¶ҲзҒӯзҷҢ
иғ¶иҙЁзҳӨж–°и‘Ҝ
ONC201жҳҜеӨҡе·ҙиғәD2/3еҸ—дҪ“пјҲDRD2/3пјүзҡ„йҖүжӢ©жҖ§жӢ®жҠ—еүӮпјҢиғҪеӨҹжңүж•Ҳең°йҖҸиҝҮиЎҖи„‘еұҸйҡңпјҢеҸӘж¶ҲзҒӯзҷҢ
 жҖҘжҖҘжҖҘпјҢжұӮж–№жЎҲпјҢеёҢжңӣеҫ—еҲ°еӨ§е®¶зҡ„её®еҠ©
зҫӨйҮҢзҡ„иҖҒеёҲ们пјҢиҜ·й—®еҰӮжһңиӮҫиҪ¬з§»дјҡе·Ұдҫ§и…°д»ҘдёҠз—ӣеҗ—пјҹе·Із»Ҹз—ӣдәҶжңүеҚҠдёӘеӨҡжңҲгҖӮдёҖејҖе§Ӣз—ӣзҡ„ж—¶еҖҷ
жҖҘжҖҘжҖҘпјҢжұӮж–№жЎҲпјҢеёҢжңӣеҫ—еҲ°еӨ§е®¶зҡ„её®еҠ©
зҫӨйҮҢзҡ„иҖҒеёҲ们пјҢиҜ·й—®еҰӮжһңиӮҫиҪ¬з§»дјҡе·Ұдҫ§и…°д»ҘдёҠз—ӣеҗ—пјҹе·Із»Ҹз—ӣдәҶжңүеҚҠдёӘеӨҡжңҲгҖӮдёҖејҖе§Ӣз—ӣзҡ„ж—¶еҖҷ
 йә»зғҰжҺЁиҚҗдёҠжө·иӮҝзҳӨеҢ»йҷўеҒҡиӮҫи„ҸжүӢжңҜзҡ„еҢ»
зҲ¶дәІиҝҷдёӨеӨ©еҒҡctеҸ‘зҺ°жңүиӮҝзү©пјҢеҢ»йҷўеҲқжӯҘеҲӨж–ӯдёҚеӨӘеҘҪпјҢеҸҜиғҪйңҖиҰҒеҒҡжүӢжңҜпјҢжұӮеҗ„дҪҚжҺЁиҚҗдёҠжө·иӮҝзҳӨ
йә»зғҰжҺЁиҚҗдёҠжө·иӮҝзҳӨеҢ»йҷўеҒҡиӮҫи„ҸжүӢжңҜзҡ„еҢ»
зҲ¶дәІиҝҷдёӨеӨ©еҒҡctеҸ‘зҺ°жңүиӮҝзү©пјҢеҢ»йҷўеҲқжӯҘеҲӨж–ӯдёҚеӨӘеҘҪпјҢеҸҜиғҪйңҖиҰҒеҒҡжүӢжңҜпјҢжұӮеҗ„дҪҚжҺЁиҚҗдёҠжө·иӮҝзҳӨ




 жҳҫиә«еҚЎ
жҳҫиә«еҚЎ

